Stat 414 – Review Problem Solutions
(F24)
Let me know if you spot errors
or want an answer elaborated on!
1) Plots
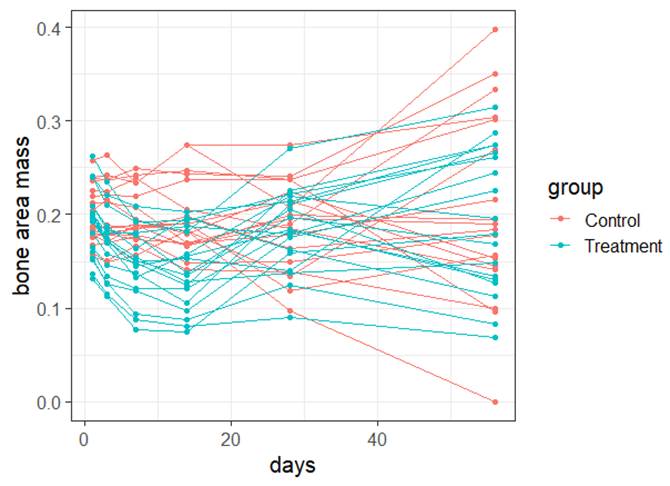
(a)
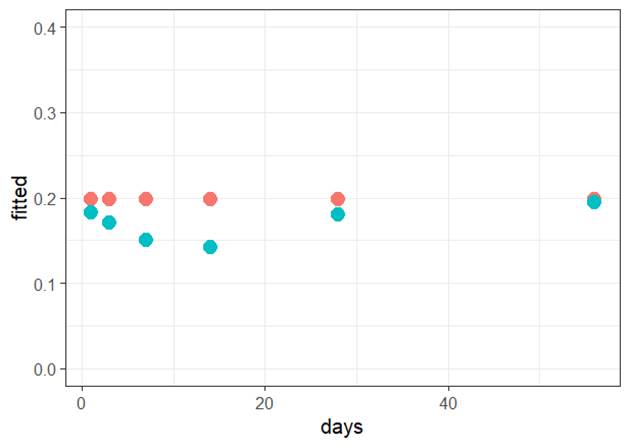
Form of the model: Because the residuals vs. fits graph does not show any leftover pattern, the
form of the model I used appears to be adequate.
Independence: We have repeated observations on the same mouse so
independence is violated.
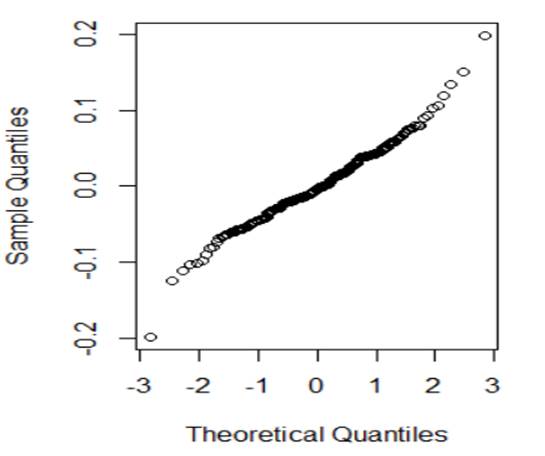
Normality:
The normal
probability plot looks reasonably linear, so the normality of the errors
condition is met.
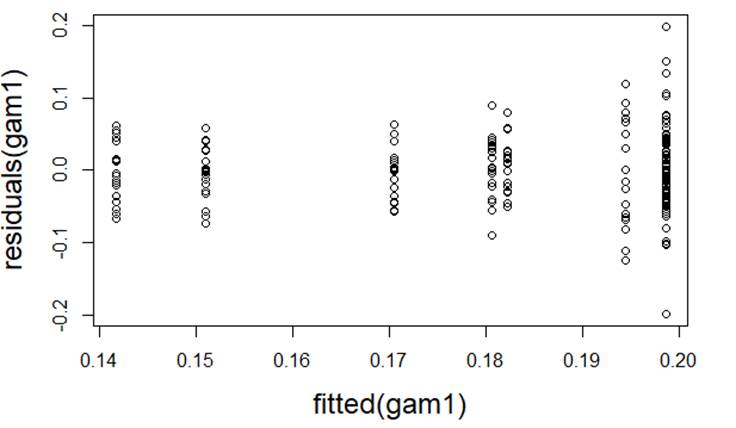
Equal
variance: The residuals vs. fits graph shows
increasing variability in the residuals with increasing fitted values,
indicating a violation of equality of the error variances at each x (though not super severe)
(b)
Which of the following would you consider doing next to improve the validity of
the model? Briefly justify your choice(s).
·
Transformation
to improve linearity No, model form was fine.
·
Quadratic
model to improve linearity No, model form was fine
·
Transformation
of response to improve normality No, normality was
fine
·
Transformation
of explanatory to improve normality No, normality was
fine
·
Include
days as a variance covariate Yes, the variability in the residuals appears to increase
with the number of days
·
Include
group as a variance covariate No, the variability in the two treatment groups appears
reasonably equal
·
Multilevel
model using mouse as a grouping variable (Level 2 units) Yes, this will allow us to model the repeat observations over time as
well as on each mouse (two knees)
2) Here is another model for the FEV data
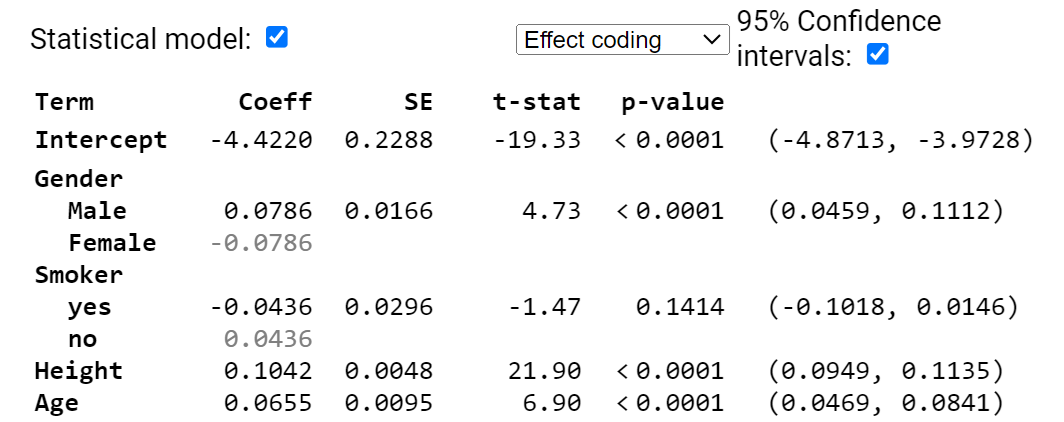
(a) Provide a rough estimate of a 95%
confidence interval for a 17-year-old male smoker who is 64 inches tall.
First, we predict a
17-year-old male smoker, 64 inches
![]() liters
liters
Then a rough standard error
around this prediction (for an individual) is 2 * residual standard error. Where do I find the residual standard error
in the above output? ![]() = .412
= .412
I am 95% confident that an
individual with these characteristics will have an FEV between 2.58 and 4.22.
From R

(b) Interpret the (0.0459, 0.1112)
interval in context.
We are 95% confident that,
after adjusting for height, smoking status, and age, the average FEV of males
is 0.0459 to 0.112 liters higher than average (or about .09 to .22 liters
higher than the females average of the same age, height, and smoking status).
Note, with this “complete output” I can see that both Smoker and
Gender are using effect coding.
(c) Smoker doesn’t appear to be
significant in this model. Explain two
ways I can tell this?
The confidence interval
for the smoking effect contains zero and the p-value for smoker is larger than
.05.
(d) Can I just remove the smoker
variable from the model?
(d) Can I walk away saying “smoking
status is not related to FEV?
No, this only says Smoker
variable is not useful after adjusting for the other variables. In combination
they may explain much of the variation that Smoker was explaining. This doesn’t
say smoking status isn’t related to FEV, just that it doesn’t improve the
predictions significantly if we already know height, age, and gender.
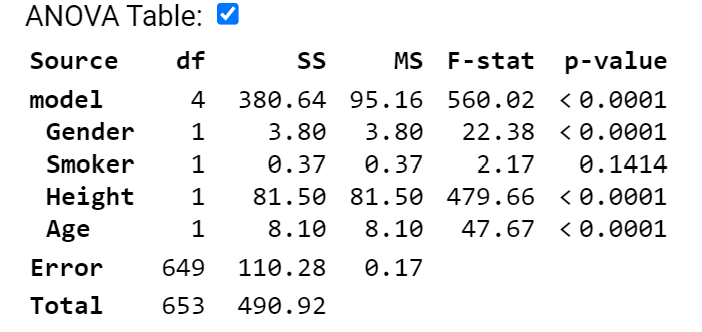
(e) State the null and alternative
hypotheses for removing Smoker from the model. Is the p-value for this test in
the above output?
![]()
![]()
Because this is a binary
variable, we can use either the t-statistic p-value (.1414) or the
F-statistic p-value (.14.14), they will match.
Both of these are after adjusting for all other variables in the
model. Watch for
-
ANOVA output using sequential sums of squares
-
Categorical variables with more than 2 categories where we would
have to use the partial F-test, rather than the t-test.
Also remember that this is
not the p-value for testing “is smoking related to FEV”
(f) If I remove the height
variable, smoker is now significant at the 5% level. What does this tell you?
This tells us that
removing height changes the se residuals (expect to increase) and the
coefficient of smoker (if it’s now significant with a smaller residual standard
error, then it increased). But by the coefficient of smoker changing, that
tells us there is also a relationship between height and smoking status in this
dataset.
Example R output with
indicator coding.
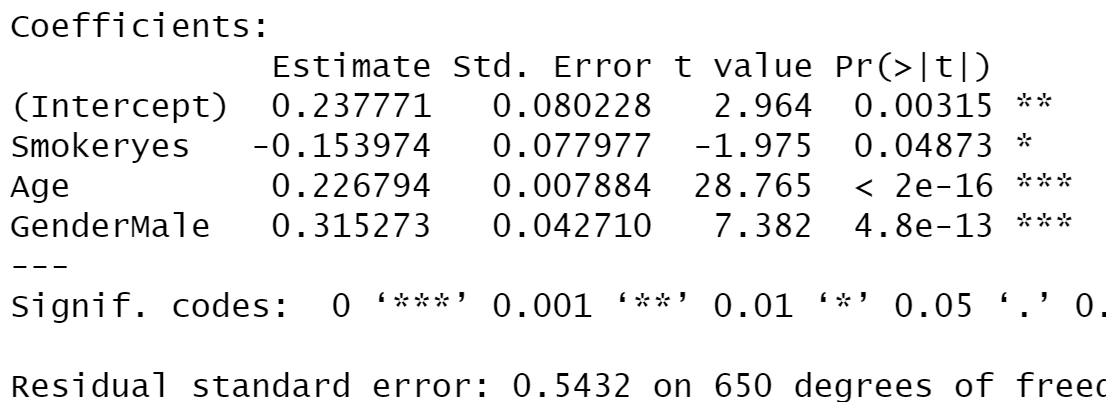
When we take out height,
smoker because a proxy for taller (and older) people
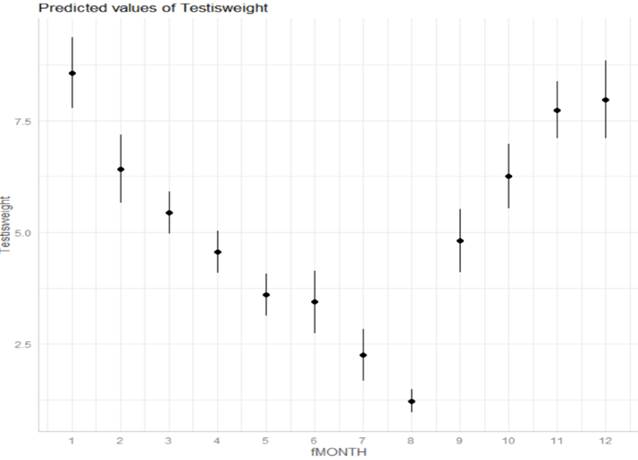
3) Squid data
(a) Is there
seasonality in the data?
We
do see evidence in the boxplots that the median Testisweight varies noticeably
across the months suggesting seasonality.
(b) Does the
variability in the response appear to vary by month? Identify 3 months where
you think our predictions of Testisweight will be most accurate. Least?
We
also see evidence in the boxplots that the box widths differ noticeably across
the months, suggesting unequal variances in the Testis weights among the
different months. Months 7 and 8 has less variation (more accurate) and Months
9 and 10 seem the least accurate.
(c) If this
model was fit with indicator coding and fMONTH = 1 as the reference group, is
the coefficient of fMONTH2 positive or negative?
Month 2 is lower than Month
1 so the coefficient will be negative.
(d) If this
model was fit with effect coding, is the coefficient of fMONTH2 positive or
negative?
Month 2 is above average,
so the coefficient will be positive.
(e)
Continuing (d): If fMONTH1 is the missing category, will its coefficient be
positive or negative?
Month
1 is above average, so the coefficient will be positive. Or if we had displayed
all the other coefficients, we could sum them together and see the sum comes
out negative.
But for
addressing the unequal variance: We don't want to assume a "linear
relationship" between the variability in the residuals and month number,
so we will estimate the variance for each month. We can do that by finding the
sample variance for each month.
(f) Which
months do we want to 'downweight' in estimating the model?
The
months with more variability, e.g., months 9 and 10.
(g)
Conjecture what changes you would expect to see in the previous two graphs in
this weighted regression model.
Now
we are going to let the variances vary by month, so the graph of the fitted
model would have much larger SEs for months 9 and 10, and smaller for months 7
and 8.
(h) How do
you expect the residual standard error to change in the weighted regression
model?
We
expect months 7 and 8 to have pretty small ![]() values and then the other months will be
multipliers for based on the larger month SDs.
The small
values and then the other months will be
multipliers for based on the larger month SDs.
The small ![]() corresponds to a smaller residual standard
error.
corresponds to a smaller residual standard
error.
4) AirBnb
(a) Level 1 = AirBnB listing; Level 2 =
neighborhood
(b) Level equations
Level 1:![]()
Level 2: ![]()
and ![]()
(c)
Which do you expect to be larger ![]() or
or ![]() ? Explain your
reasoning.
? Explain your
reasoning.
Conceptually we might expect
more variation in prices between listings in the same neighborhood but maybe
less variation in the mean price listings across neighborhoods.
(d)
Interpret the intercept coefficient in context.
The intercept ($25.35) is
the predicted price for a listing for the entire house/department with 0
satisfaction rating in the average neighborhood.
(e)
Interpret the coefficient of overall_satisfaction in context.
A one-point increase in the
overall satisfaction rating, after adjusting for neighborhood and room type, predicts a $24.92
increase in the (average) price.
(f)
Based on this output, is the type of room statistically significant? State the null and alternative hypothesis in
terms of regression parameters, and clearly justify your answer.
![]()
![]()
Using the partial F-test from
the ANOVA table, the p-value is very small because the F-statistic is very
large (244.195)
(g) Consider the following two variables:
PctBlack would allow a more
“granular” look at the relationship, the rate of decrease in predicted price
with each additional percentage point, BUT, that relationship would need to be
linear. Look at a graph before adding
PctBlack into the model. If the relationship isn’t linear, then using the
binary version could be an alternative.
I am assuming that prices decreases with increasing percentage black in
the neighborhood so predict a negative coefficient (including for the binary
variable as 1 corresponds to the higher percentage).
(h) If HighBlack is added to the model
how/if do you expect ![]() or
or ![]() to change? Explain
your reasoning (for each).
to change? Explain
your reasoning (for each).
This is a Level 2 variable
so we don’t expect ![]() to change but do expect
to change but do expect ![]() to decrease.
to decrease.
(i) Consider the first few observations of
the first row of the variance-covariance matrix for the above model output
![]()
Where will the first zero
value occur?
Depends how many
observations there are in the first neighborhood. If that number is K, then K+1 through the
1561 columns of that first row will be zero, as those would all be other
neighborhoods and we are assuming observations in different neighborhoods are
not correlated.
(j) Here is the first row of the
corresponding correlation matrix
![]()
Verify the value for 0.0861.
487.0952/(5657.442) = .086
(k) If I were to look at the first row of
the corresponding correlation matrix for the null model, how do you think the
second value will compare? (likely) Explain your reasoning.
Typically (but not always), the
within-group correlation will be larger in the model that doesn’t explain any
of the Level 1 and Level 2 variability.
5) Which model demonstrates more school-to-school variability
in language scores?
On average, the slope
coefficients are larger in magnitude for the modelling including IQ_verb. It’s counter intuitive, but in this case,
after adjusting for IQ_verb, there is actually more school-to-school variation. The main cause is that within school and
between school relationships are not consistent, schools with lower language
scores tended to have higher IQ_verb scores, so after adjusting for IQ_verb,
the “additional contribution” to match the school means is larger.
6)
Consider this
paragraph: The multilevel models we have considered up to this point control
for clustering, and allow us to quantify the extent of dependency
and to investigate whether the effects of level 1 variables vary across
these clusters.
(a) I have
underlined 3 components, explain in detail what each of these components means
in the multilevel model.
Control for clustering: We have observations that fall into natural groups and we don’t
want to treat the observations within the groups as independent, by including
the “clustering variable” in the model, the other slope coefficients will be
“adjusted” or “controlled” for that clustering variable (whether we treat it as
fixed or random)
Quantify the extent of the
dependency:
The ICC measures how correlated are the observations in the same group
Whether the effects of level
1 variables vary across the clusters: random slopes
(b) The multilevel model referenced in
the paragraph does not account for “contextual effects.” What is meant by that?
The ability to include Level
2 variables, variables explaining differences among the clusters. In particular, we can aggregate level one
variables to be at Level 2 (e.g., group means). Being able to include these in
the model, along with controlling for the individual groups, is another huge
advantage of multilevel models.
7) Give a short
rule in your own words describing when an interpretation of an estimated
coefficient should “hold constant” another covariate or “set to 0” that
covariate
We should hold variable 2
constant (which can include random effects) when we are interpreting the slope
of variable 1.
We should put all explanatory
variables (including the Level 2 random effects) at zero when interpreting an
intercept. In a random intercepts (only)
model, all the slopes are the same so you can say “in a particular school”
8) SAS output
(a)
What is the patient level variance? (Clarify any assumptions
you are making about the output/any clues you have.)
Because the
first table is titled “covariance,” I’m assuming those are estimated variances
rather than estimated standard deviations.
The patient to patient variance is estimated to be ![]() = 73.7 mmHG2 (within the same
clincial center)
= 73.7 mmHG2 (within the same
clincial center)
(b)
What is the center level variance?
The center
to center variance is estimated to be ![]() = 10.7 mmHG2
= 10.7 mmHG2
(c)
What is an estimate of the ICC? Calculate and interpret.
10.7 / (10.7
+ 73.6) approx 0.13. This represents the
correlation btween two patients at the same clinic and that 13% of the
variation in diastlic blood pressure is at the clinic level.
(d)
What is the expected diastolic blood pressure for a randomly
selected patient receiving treatment C at a center with average aggregate blood
pressure scores?
90.97 mmHG, the
intercept (no treatment C effect and no clinic effect because at the average
center)
(e)
What is the expected diastolic blood pressure for a randomly
selected patient receiving treatment A at a center with aggregated blood
pressure scores at the median?
Because we are
assuming the clinic effects are normally distributed, with a center at the
median, ![]() is again assumed to be zero. So 90.87 + 3.11 to include the effect of
treatment A = 93.98 mmHG.
is again assumed to be zero. So 90.87 + 3.11 to include the effect of
treatment A = 93.98 mmHG.
(f)
What is the expected diastolic blood pressure for a randomly
selected patient receiving treatment C at a center with aggregate blood
pressure scores at the 16th percentile?
Now we want
to assume the clinic effect is 1SD below zero where the random clinic effects
are assumed to be normally distributed with mean zero and standard deviation =
sqrt(10.67). So a clinic at the 16th percentile is predicted to fall 3.27 below
the average across all the clinics.
So 90.87
(intercept) + 0 (treatment C) – 3.27 (random effect for 16th
percentile) = 87.60 mmHG.
(g)
What is the expected diastolic blood pressure for a randomly
selected patient receiving treatment B at a center with aggregate blood
pressure scores at the 97.5th percentile?
Now we want
to assume the clinic effect is 2SD above zero = 2(3.27)
So 90.87 +
1.41 + 2(3.27) = 98.82 mmHG.
9) For a sample of 400 children from the National Longitudinal
Survey of Youth, we have data on the child’s cognitive test score at age 3
(“ppvt”), the mother’s level of education, and the mother’s age at the time she
gave birth.
Below are the graphs and output related
to regressing the ppvt score on the mother’s age
For each assumption below, comment on
whether you think it is met. Explain how you are deciding or what additional
information you would need. If you think the assumption is violated, explain
the nature of the violation.
(a) (2 pts) Linearity The Residuals vs. Fitted graph shows only minor curvature
(the red smoother is almost flat) indicating that the linearity assumption is
satisfied (removing the linear components leaves random scatter rather than a
pattern)
(b) (2 pts) Equal variance The Scale-Location graph does show a slight downward
trend (showing a gradual decrease in the overall magnitude of the residuals as
shown a bit by fanning in in the Residuals vs. Fitted graph as well) but the
largest SD does not appear to be more than twice the size of the smallest SD so
I could consider this condition sufficiently met.
(c) (2 pts) Normality We would need a graph (histogram or normal probability
plot) of the residuals
(d) (2 pts) Independence We were told this was a
professional collected sample so if we consider it a random sample from the
population of interest, with no repeat observations are even multiple children
from the same family, then the independence condition is met. If they were cluster
sampled from different neighborhoods, then we might have some concerns.
For same dataset, model
10) (a) (3 pts) Provide a one-sentence interpretation of the
following output
predict(model4, newdata = data.frame(momage=30), interval = "prediction")
fit lwr upr
1 95.89836 56.38459 135.4121
I’m 95% confident that a
single 30-year old mom will have a child with ppvt score between 56.4 and
135.4.
(b) (2 pts) Suppose instead we used interval = "confidence"
1. Identify one thing that will not change
The midpoint (“fit”) of the interval will not change.
2. Identify one thing that will change
The width of the interval will be much smaller because now it’s
an interval for the population of pvt scores for all children with mom age = 30
years.